Otosclerosis
What is Otosclerosis?
It is also known as Otospongiosis. It is a disorder of bone remodeling limited to the enchondral layer of the capsule of the inner ear. This disorder is limited to the temporal bone only.
Bone is in a constant state of flux and is constantly being remodeled. In the inner ear bone remodeling is much slower as compared to that of the bones of the rest of the body. However a trigger is initiated which causes faster bone remodeling to occur in the inner ear.
There are two phases.Active phase: In this situation the bone becomes soft and spongy and is very vascular.
Inactive phase:The bone becomes sclerotic and hard, resulting in the name “otosclerosis”.
The new bone formation prevents the stapes bone from vibrating causing it to get “fixed” and is thus no longer able to transfer (conduct) sound to the inner ear thus resulting in deafness.
What causes otosclerosis?
In recent times measles is thought to be responsible for causing otosclerosis. The person contracts measles which can then later on cause otosclerosis.
Hereditary ( “inherited”) genes are also identified as a cause.
It was thought that fluoride deficiency in water could result in the formation of “otosclerosis”.
How does otosclerosis present?
The person suffering from Otosclerosis will initially suffer from deafness. This is likely to be a conductive deafness. But on occasion it can present as nerve deafness or as a combination of nerve and conductive deafness known as mixed deafness.
The deafness initially manifests itself very gradually around the age of 20 and then gradually progresses. It mostly occurs in both ears simultaneously. Women are commonly affected and the deafness is first noticed after the first pregnancy.
Other symptoms that can occur are tinnitus (a constant humming sound), a feeling of the ear being blocked. Giddiness (vertigo) can also be present.
What are the tests needed to confirm that the patient is suffering from otosclerosis.
Otosclerosis is a clinical diagnosis, that is to say the ENT physician by listening to the patients history, complaints and from a careful examination can then conclude that the patient if suffering from otosclerosis.
There are tests that are typical of otosclerosis. They are- Pure tone audiogram: Usually shows a conductive hearing loss with a dip at 2 KHz , known as Carharts notch.
- Speech audiometry shows very good speech discrimination scores.
- Impedance (immitance) audiometry shows the following, (a) Low compliance (Termed an As peak), (b) stapedial Reflexes are absent and (c) Normal middle ear pressure.
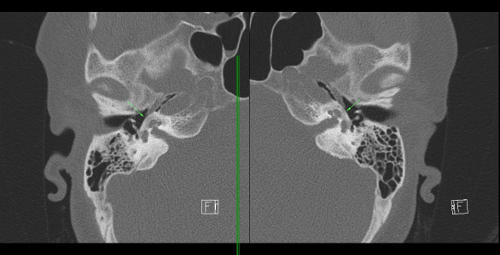
- High resolution CT scanning of the temporal bones in recent times are useful especially in the active phase in detecting areas that are affected by otosclerotic foci.
What are the treatment options of Otosclerosis?
- Hearing Aids: These offer significant benefit and the patient can hear well using these. The advantages are (a) Excellent hearing, (b) no risk of hearing loss that accompanies surgery. Disadvantages: (1) Hearing Aids are expensive, (2) Batteries need to be replaced, (3) Most insurance companies do not pay for hearing aids, (4) External ear infections as the result of the usage of hearing aids.
- Surgery: This is usually termed stapedectomy. A stapedectomy is an operation whereby the stapes bone is replaced by a prosthesis that replaces the functioning of the stapes bone. The stapes is removed and an opening (termed ‘fenestra”) is made in the oval window. A prosthesis is then placed on the incus and into the new opening (fenestra). The opening is usually sealed by connective tissue or a by a vein graft to prevent leakage of inner ear fluid (known as perilymph) from leaking out. A well done stapedectomy results in excellent hearing. Complications of stapedectomy are
- Permanent irreversible hearing loss. This is a real and genuine complication even when performed by a senior and experienced ENT surgeon. It can result even if the surgery has been done flawlessly. Most surgeons give the incidence of permanent nerve hearing loss following stapedectomy as approximately 5% of the time with 95% of the time the surgery resulting in excellent hearing. Permanent irreversible sensorineural hearing loss can occur immediately or gradually over time
- If the nerve known as the chorda tympani gets cut it can result in loss of taste
- Facial nerve paralysis. This can be transient (temporary) or very rarely it is permanent.
- Perilymphatic fistula: This is a feared complication. This occurs when fluid from the inner ear drips out of the inner ear through the opening made in the oval window. Signs typical of perilymphatic fistula are (i) Severe vertigo, (ii) Tinnitus, (iii) Fluctuating hearing loss. Perilymphatic fistula needs to be treated urgently and requires immediate closure.
Lasers in stapedectomy
Lasers have reduced complications but not eradicated them. Lasers make surgery less traumatic and have reduced the need for manual force.
Right Ear - Coronal

Left Ear Axial